HYPOGLYCEMIA MIMICKING STROKE
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/ guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box are welcome.
Here is a case I have seen:
A 65 year old woman, weaver presented to casualty at 7: 30 am with the complains of :
Right upper limb weakness since 4am
Right lower limb weakness since 4am
Slurred speech since 4 am
Patient used to work as a weaver until 2 years back. She got married to a weaver and has 5 children - 3 daughters and 2 sons. Her attendants give a long standing history of fever since 10 years on and off though it wasn't associated with weight loss. 5 years ago, she was diagnosed to be hypertensive and diabetic on routine check up and is on OHAs and Anti hypertensive medications ever since. She has been on Tab Glimiperide 1mg once a day, Tab Gliclazide 60mg once a day and Tab Cilnidipine 10mg OD. Since 4 years she has been admitted twice at OMNI hospital for ? LRTI and since 4 years the attendant tells that she has been having fever along with productive cough on and off though she hasn't been evaluated for Pulmonary Kochs. She was put on Oseltamavir, N-acetylcysteine and Monteleukast. In 2017, an Upper GI endoscopy was performed which showed normal study as she complained of epigastric pain and indigestion. Her reports from Dec 2019 shows albuminuria for 3 plus and with a serum creatinine 2 mg/dl with grade 1 RPD changes. Also, she started to complain of hard stools and was diagnosed with hemorrhoids in an outside hospital for which she has been using a syrup.
Her attendants tell us that she has gained weight over the last 6 months and eats only one meal a day since 3 years.
On 10/8/2020,
The attendants heard a cry at 4 am and when they went to check on the patient they noticed that the patient couldn't get up from her bed and was having difficulty in speech. They took her to a nearby hospital where they were told that she had high blood pressure of 160/100 mmhg and was given Tab Amlong 5mg.
The patient presented to our casualty at 7:30 am.
General Examination:
The patient was conscious and coherent. She was obese, appeared pale, and bilateral pedal edema was present. She had a slurred speech and was complaining of right upper and lower limb weakness.
Vitals: Afebrile, BP: 150/100, Pulse: 67 bpm, RR: 17 cpm, Saturations at 98 %, GRBS: 40 mg/dl
Pallor +
No H/O icterus, cyanosis, clubbing, and lymphadenopathy

Systemic Examination:
CNS Examination:
Higher motor functions are normal
All cranial nerves are intact
Tone is normal in all the limbs on both sides.
Power:
Her Left UL and LL showed a power of 4/5 and 3/5 respectively. Though she had only flicker movements in her right upper and lower limbs.
Reflexes: Right Left
Biceps 4+/5 4+/5
Triceps 4+/5 4+/5
Supinator 4+/5 4+/5
Knee Absent 3/5
Ankle Absent Absent
Plantars Flexion Flexion
CVS Examination:
S1 S2 heard
No murmurs
Respiratory Examination:
Her lungs are clear on auscultation
Bilateral air entry present
No added sounds
Abdomen on palpation - Multiple painless lipomas could be palpated, mobile in the right hypochondriac, right lumbar region - Dercums disease ( Multiple, painful, fatty benign lipomas chiefly in obese, post menopausal women).













Course in the hospital and disease discussion
On Day 1,
The patients blood sugars were maintained within the normal range with the help of 25 % dextrose infusion.
Fundoscopy was done to look for any diabetic or hypertensive retinopathy changes which showed Grade 1 hypertensive retinopathy in both her eyes.
HER BLOOD SUGAR MONITORING ON THE DAY OF ADMISSION

By Day 2, the patient was tapered off 25 % dextrose infusion
The blood sugars were well maintained without the need for 25% dextrose
Only her biceps reflex was exagerrated bilaterally
By Day 3,
The patient was able to walk with support, she says she is able to walk just like before
Her BP was at 150/100mmhg
With a PR of 70bpm
Problem Representation :
66 year old woman with Right Upper limb and Lower limb weakness and slurred speech since 3 hours due to hypoglycemia
1.Recurrent Hypoglycemia ( resolved) secondary to Sulfonylureas on Renal failure 2. ? HFpEF with Ef - 64 % 3.Kco CKD since 1 year ( eGFR - 34mL/min/1.73 m2) 4. Kco Type 2 DM and HTN With Grade 1 Hypertensive Retinopathy changes 5. Cholithiasis since 2 years - Asymptomatic 6. ? Iron Deficiency anemia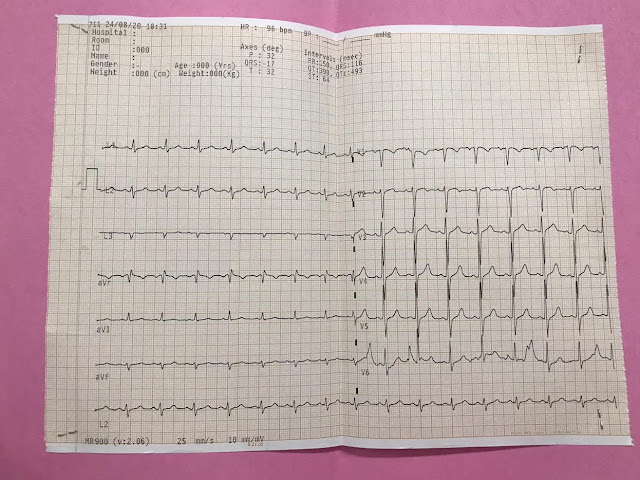

Comments
Post a Comment